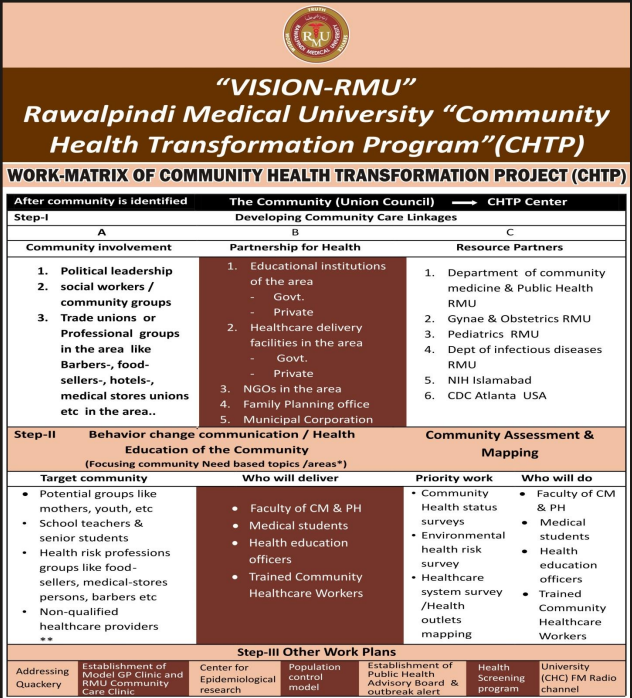
CHTP
CHTP

- Self-medication and Non-qualified Healthcare practices or Quackery:

- In USA, more than 20 groups of drugs are allowed for over the counter sale including pain killers, antihistamine and H-2 receptors blockers etc. It reveals that healthcare is not possible to deliver in tight boundaries of medicine even in affluent countries. We have different population which has its own limitations and potentials.
- Self-medication or medications taken on advice of non-qualified persons (Quacks) or healthcare obtained from non-qualified sources are very frequent happenings in our society. Measures taken against such malpractices have not proven effective. Primarily it is people’s faith & acceptance for such malpractices for reasons like low literacy and low paying capacity.
- An effective intervention would be behavior change communication for both groups. It is the time to regulate this phenomenon. We have to develop our own model under our health issues, our population profile and the resources available. In fact such non-qualified sources exist very deeply and frequently. Factually, quacks or other non-qualified healthcare sources also serve as first level of contact for a big proportion of our population in times when medical care is warranted. They are the readily available & easily accessible (socially, geographically & economically) healthcare sources to the people. While addressing this issue at one end, people need to be informed & educated against hazards of such practices’. on many aspects including allowing them limited use of self care medicinal measures, also hazards of using nonqualified medical services. At the other end, non-qualified persons may also be involved purposively. It is purposed that persons who meet certain standards like trained dispensers, nurses, mid-wives, technicians, and in relatively younger age group etc) may after imparting some relevant & purposively designed education & training as to restrict them to do something and to not do other things, (e.g. to whom to medicate / treat and to whom not, or timely refer ), would play role in addressing medical-care needs of such population which is currently being not served by qualified healthcare resource in govt. or private capacity. This would also bring such health outlets or persons on tax network and health department record hence would be easy to regulate & monitor. They would also be connected to govt. sector referral mechanism. Being first contact level for majority of peoples with high potential of disease development & spread their role in earlier identification of emerging health problems or outbreaks can be well appreciated. Such data would also be very rich for health research purposes.
- It is suggested that such non-qualified HCPs who meet certain criteria like age <45Y, 12grade science education, have some certified training and agreed for new role etc would be subjected to education & training focusing on following areas;
- hazards of non-qualified healthcare practices
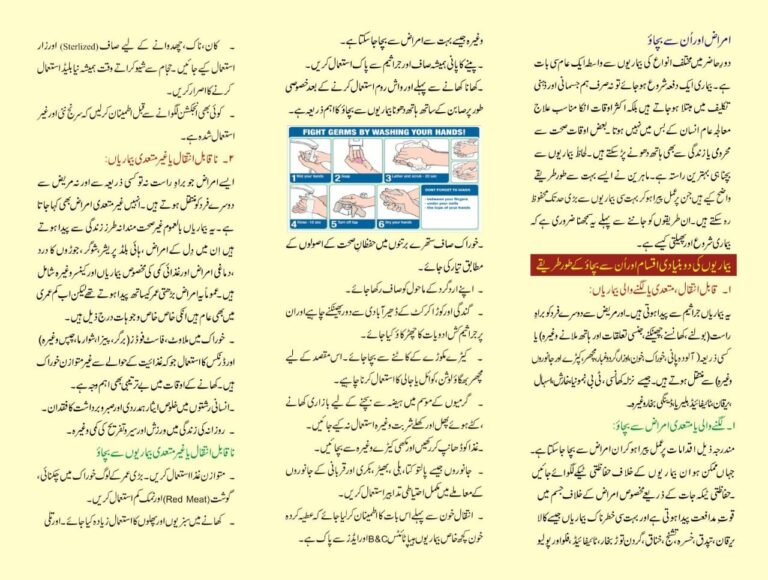
- Hazards of un-safe injection practices
- Hazards of unjustified use of drugs , antibiotics etc
- Value of timely referral of patients
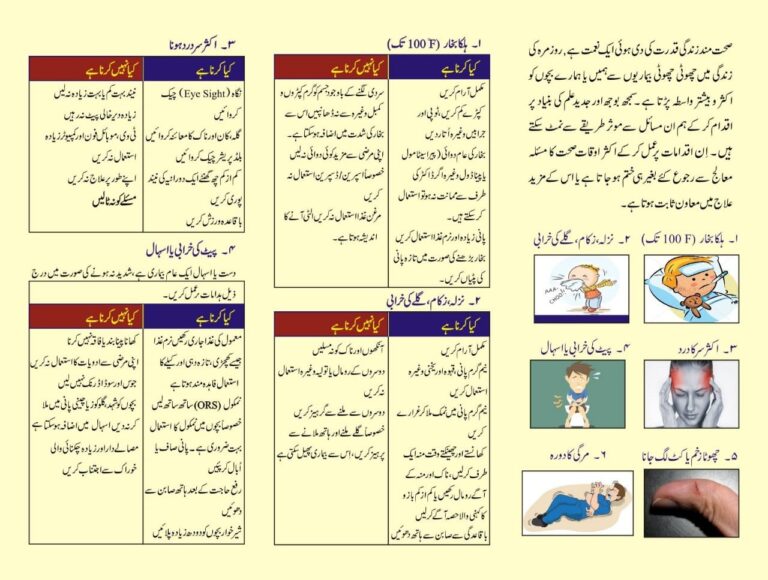
- Management of common health problems like ARI, Diarrhea, Fever and minor injury etc.
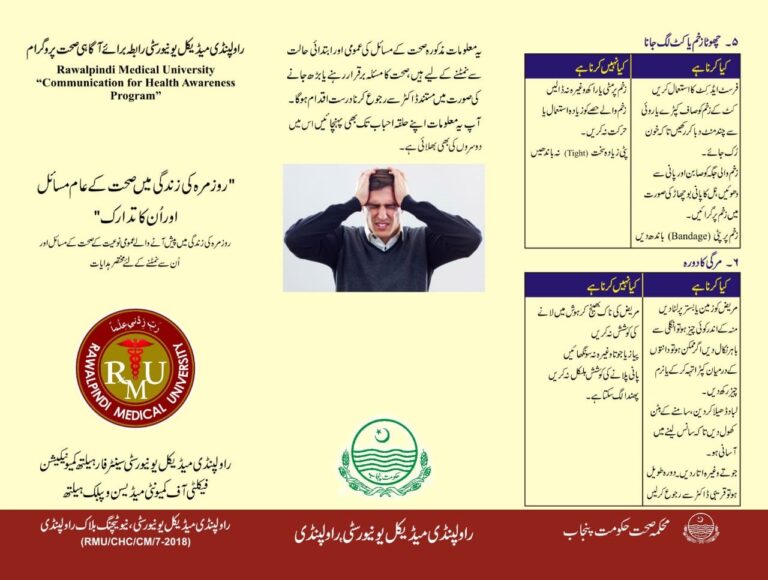
- First aid trainings like CPR, wound first aid, seizure care etc.
- Role in disease surveillance
- Standardization of Qualified Healthcare Practices (GP clinics)
- It is on Govt. agenda to regulate private health sector. This program will focus ethical and academic aspects of medical care practices. After purposively involvement of Private HCPs of the area they will be subjected to medical care improvement areas including standardization of clinical facility & practice, continuous medical education (CME), reporting health data, population control, disease surveillance and medical research etc.
- Population Control Strategy in CHTP:
- Rapid population growth is a significant national issue and major bar to national development. The issue has not been addressed effectively in spite of historical efforts. The strategy adopted in CHTP is as under;
- Healthcare providers (HCPs) of the UC will be taken on board ( DHA will be made instrumental)
- Nikah registrar of the UC will be bound to motivate, inform and guide (on paper) to each new bridegroom to see specified HCP of the UC. The area Counselor will be intermediary.
- The HCP will hold counseling session with bridegroom or couple on family planning including contraception on pre-decided guidelines. (this work of HCP & Nikah registrar may be hired on payment if DHA & MOP agrees) . Output of this male education & motivation would be measureable.
- Rapid population growth is a significant national issue and major bar to national development. The issue has not been addressed effectively in spite of historical efforts. The strategy adopted in CHTP is as under;
- University (CHC) FM Radio channel